
For the last 5 days I've been taking 5-HTP.
5-HTP is a precursor to serotonin (that is, it becomes serotonin once metabolised by the body).
I've previously used 5-HTP for experimenting with my sleep composition, and to try to reliably trigger lucid dreams. The dosage that I was taking then was 50 - 100mg at night.
This time I tried a brand that contained "co-factors". These are associated vitamins and minerals that help the body to metabolise the 5-HTP into serotonin.
I decided on 200mg each night about 10 minutes before getting into bed. 100mg is the recommended maximum daily dose of this brand, although I have seen others that give a maximum daily dose as 300mg.
I have also seen medical literature that cites doses of 150mg-300mg as a daily dose (as a trial for treating depression), so toxicity at this dose seemed unlikely.
Why did I take 5-HTP?
The rather lazy answer is that (as I mentioned above) I've taken it before without ill effect, and that it is mentioned to have a positive effect on sleep, even being cited as having a positive effect on a severe case of insomnia
A rather cheeky and over-simplified answer is that I have already shown that a depressant (alcohol) increases my AHI, so I wondered if something that has antidepressant properties would have the opposite effect and reduce my AHI.
I have also seen medical literature that suggests a link between depression and sleep apnoea (both as a cause and effect of sleep apnoea).
Depression is more complicated that just having low serotonin levels, but low serotonin does play a part. Serotonin is a neurotransmitter (it is used in the body's sending and receiving of nerve impulses), so I wondered if increasing my levels would mean that I would have stronger signals to breathe during sleep and that the muscle tone in my airways would be that much "sharper".
Okay, so how did the 5 days go?
I noticed the following effects (sleep related and non-sleep related):
- I wasn't as tired in the evenings, so went to bed later
- I found it easier to wake up
- I didn't feel as hungry during the day, generally ate once at 2pm, then didn't eat in the evening.
Throughout these experiments, I go to bed when I am tired.
I calculated my average bedtime using the Zeo data. As I am doing these 5-day comparisons on weekdays (except the alcohol test - see separate blog for that), the time that I had to wake up was the same each day, hence later to bed meant less time in bed, which oddly with the 5-HTP didn't feel like a bad thing.


I wondered if my body "needed" more sleep, afterall I am used to roughly an extra hour (and still crave more), but on two mornings of the week (Fri and Sat) I can have a bit of a lie-in if I need to but I didn't want to lie in when taking 5-HTP at night (It's Saturday and I'm typing this at 7am, after waking up at my normal weekday time of 6:30am)!
It is known that some anti-depressants can decrease the amount of REM sleep that you have, so I suspected that my percentage of REM would decrease.
As percentages, the figures do not show this. In fact they show an increase in the percentage of deep sleep, along with a slight increase in REM and wake...
However, as REM is more abundant at the end of the night, it follows that the less time one spends in bed, the less opportunity there is for REM sleep, hence my actual 5-day-mean time in REM fell by 11 minutes from my baseline of 98 minutes, although it put it more inline to the average for my age of 90 minutes.
My actual time in slow-wave sleep (deep) rose by a mean of 3 minutes. My mean deep sleep (34 minutes) is still way below the average for my age (69 minutes) but within limits, so I am pleased with this small increase.
I'm not sure if these changes are actually significant, perhaps a longer trial may reveal more?

So, even if 5-HTP didn't affect my AHI, it still had positive effects on several aspects of my sleep composition.
However, it did have a positive effect on my AHI and it was much more noticeable...
I've graphed my 5-day-mean AHI alongside the other 5-day-mean AHIs for alcohol and my baseline.

It brings my mean AHI down to a level that puts me in the "normal" category (<5 AHI = normal). Maybe this is the reason for not wanting to sleep so early and finding it easier to wake in the mornings.
For the sake of showing that this is a consistent effect, I also graphed the data on a night by night basis...

For now, this seems too good to be true:
- Lower AHI
- Normal bedtimes
- Less time in bed
- Increase in slow-wave sleep
So what now? Keep on taking the tablets?
Based on my limited data, I wouldn't dare go so far as to claim that this is a effective treatment for mild (very mild) obstructive sleep apnoea, nor would I suggest that it would work for others, but it is intriguing and does need looking at further.
It leaves me wanting to know more about the mechanism behind this effect. Yes, it's good that it has helped me as far as my AHI is concerned, but I want to know how. In a previous post, I noted that my sleep apnoea seems to be REM related. Serotonin related activity drops dramaticaly during REM sleep, so maybe the higher levels due to 5-HTP reduced that effect?
Is my pseudo-science hypothesis correct, or is there more to it than that?
I'd be interested to see if this effect carried on, or if my body got used to the 5-HTP and the effect faded.
I'd also like to try this with a lower dose of 5-HTP (after all, why take a high dose if you don't need to)? I'd also like to see if sustained-release 5-HTP is more effective.
I was planning to try the mandibular advancement device next, but after such a positive effect, I think I'll stay with 5-HTP for a while and see if I can improve on the results even more. I'd like to bring my sleep latency (time to sleep onset) down.
Yes, this is good news but I can't help feeling a little like Lizzy in "Drop Dead Fred", she knows that she's taking a pill that will stop her seeing things that others can't. Will taking 5-HTP, increasing my serotonin levels and bringing my AHI down stop me from having sleep paralysis, lucid dreams and seeing/hearing the sleep-wake border imagery that I have grown so used to?
I hope not.
I'll explain how and why I came to like sleep paralysis in an upcoming blog-post. Hopefully it may be of use to anyone that fears it as I used to.
I have to say that this is a test with a tiny sample size, and of limited duration. I am not suggesting that anybody should try this, and certainly not use it in place of recognised treatments.
I've also found that 5-HTP helped reduced residual snoring after lowering my AHI with positional therapy.
Snoring Remedies? Results for 5-HTP
 Hypnagogia Blog
Hypnagogia Blog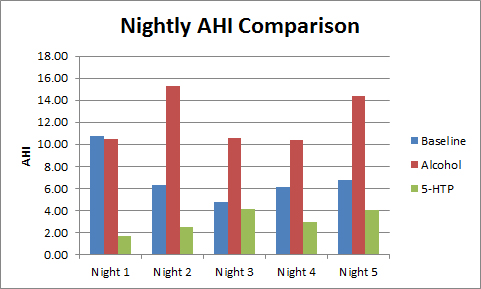
;) AHI = 9.30
AHI = 9.30

